You meant to stop ten minutes ago. You promised yourself this morning, last night, last week, the last hundred times before that. And here you are again, with the same question sitting underneath everything: why can't I stop?
That's the question almost no article actually answers. Most pivot, fast, into lists of things you should try. Keep your hands busy. Use fidget toys. Set a timer. You probably already know about those. They're not what brought you here. You came for the actual reason.
This is that article. The reason isn't laziness, weak willpower, or some character flaw. Something specific is happening in your brain, and once you can name it, the loop you've been stuck in starts to make a lot more sense. We're going to spend most of our time on the why. The how, briefly, at the end.
For a deeper grounding in skin picking disorder itself, what it is and how it's diagnosed, this overview is the foundational piece.
Key takeaways
- Skin picking has a clinical name: excoriation disorder. It's been a recognized condition in the DSM-5 since 2013, classified alongside OCD.
- Around 3.45% of adults meet criteria for it, roughly 1 in 29, with women affected slightly more than men (Farhat et al., 2023).
- The behavior is driven by brain circuits for habit and reward, not by lack of willpower. Your prefrontal cortex (the deciding part) loses to your basal ganglia (the habit part) once the loop is established.
- It commonly co-occurs with anxiety, depression, ADHD, OCD, and autism, and tends to function as self-soothing or sensory regulation.
- Shame about picking increases picking. Naming this loop is the first move out of it.
- Recovery is real. Habit Reversal Training (HRT) has the strongest evidence base.
The short answer
You can't stop the way you've been trying because the part of your brain that decides to stop and the part that actually picks aren't the same part. Picking has been moved out of the deciding part of your brain and into the automatic part, the same circuitry that runs walking, driving familiar routes, brushing your teeth. That's why you can be mid-pick before you notice. That's why telling yourself "stop" doesn't land. You're sending the instruction to the wrong department.
There's a second reason. Picking does something for you. Not something you'd choose if other options were easier to reach, but something real. A brief drop in tension. A focus when your brain feels scattered. A small, repeating dose of relief or stimulation. Your brain has logged that benefit and learned to reach for it automatically when it needs regulating. The loop runs whether you approve of it or not.
So the question "why can't I stop" has two layers. Your brain has stored this behavior in a place willpower doesn't reach. And it's still getting something out of it. Both of those are fixable, but neither responds to "just decide to quit." Which means you haven't failed. You've been using the wrong key on the wrong lock.
It's a recognized condition with a name
The behavior you're describing has a clinical name: excoriation disorder, also called skin-picking disorder or dermatillomania. The American Psychiatric Association officially added it to the DSM-5 in 2013, placing it in the obsessive-compulsive and related disorders category (APA, 2013). Before 2013, it had been described in medical literature for over a century but lacked formal recognition, which is one reason so many people who have it have never heard the word.
It's also more common than most people realize.
A separate U.S. survey of 10,169 adults by Grant and Chamberlain (2020) found 2.1% currently meet criteria and 3.1% have met them at some point in their lives. You are not a rare case. You're part of a population large enough to fill stadiums and small enough that most primary care providers still miss it.
Onset is usually in adolescence, with a peak around age 13, and the average person with it has lived with it for roughly 20 years before getting any treatment (Grant et al., 2022). Most never get treatment at all. That's not a personal failure, that's a systemic gap.
The neurology in plain English
Two main brain systems are doing the work when you pick.
The first is the prefrontal cortex, the part of you that makes plans, weighs consequences, decides "I'm not going to do this anymore." It's the part you identify with when you think "I want to stop." It's slow, deliberate, and effortful.
The second is the basal ganglia, a set of structures deep in the brain that handle habits and automatic motor programs. Once a behavior is repeated often enough, the basal ganglia takes it over. From that point on, the action runs without the prefrontal cortex needing to be consulted. This is how you can drive home from work while thinking about something else entirely. The route is in your basal ganglia.
Skin picking gets stored in the same place. The first time you picked, your prefrontal cortex was probably involved. By the thousandth time, the basal ganglia is running the program. You don't decide to start. Your hand is already there. By the time the prefrontal cortex notices and says "wait," significant damage may already be done.

Now layer reward on top. When you pick, your brain releases a small dopamine signal. Dopamine isn't pleasure exactly, it's more like the chemistry of "this is worth doing again." Neuroimaging research on body-focused repetitive behaviors has identified differences in reward-processing regions including the dorsal and ventral striatum, areas central to habit formation and reward (Grant et al., 2022). Picking delivers a brief regulation effect: tension drops, scattered attention narrows, the body finds something to do. Your brain encodes that and reaches for it more readily next time.
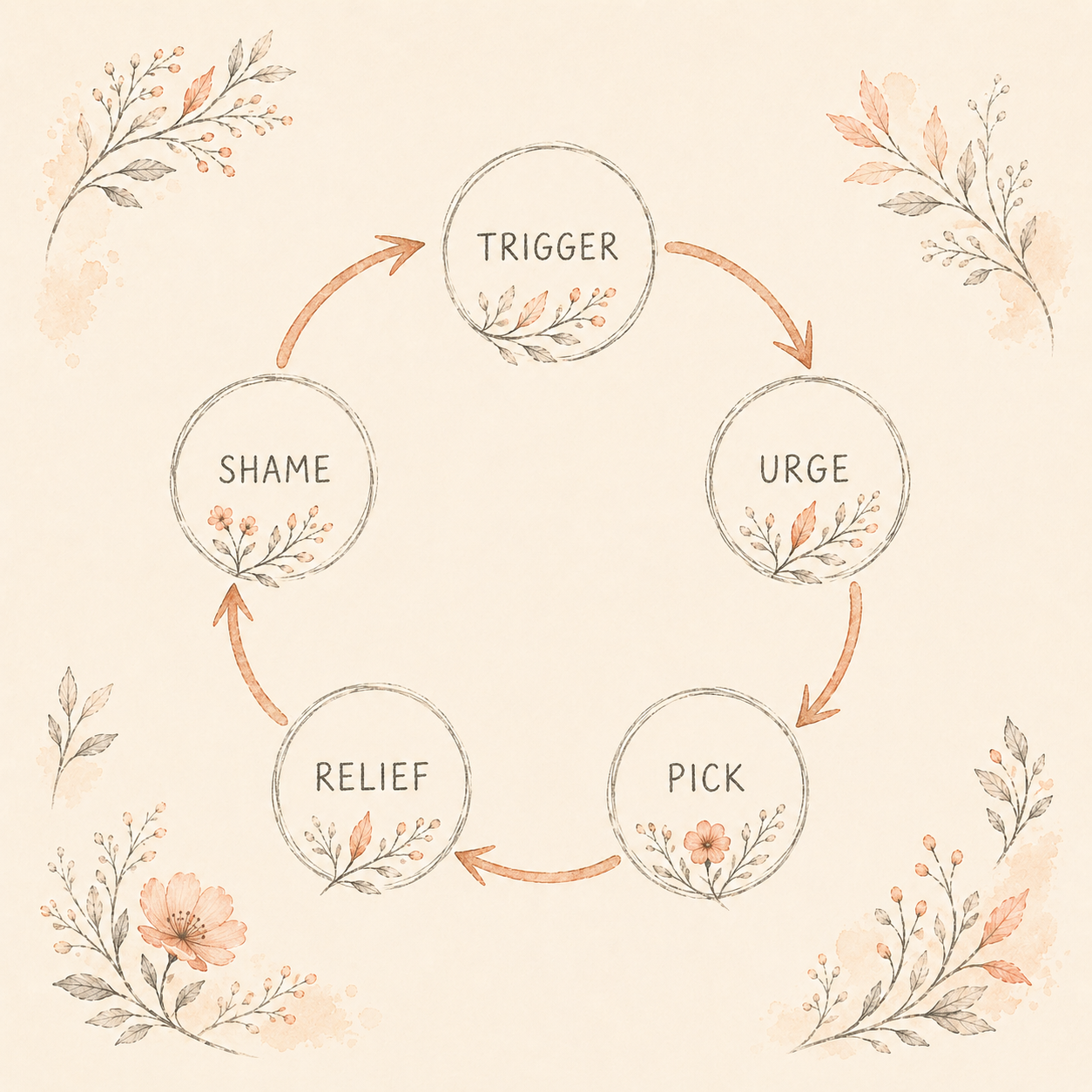
This produces what researchers call the urge-action loop. A sensation rises, sometimes physical (an uneven texture, a bump), sometimes emotional (boredom, anxiety, restlessness). The urge to pick spikes. You pick. The urge falls. Relief, briefly. The loop closes. Run that loop enough times and it becomes the brain's default response to that family of sensations.
The strategies that work for picking are the ones that address the urge before the loop fires, replace the action with something that delivers similar regulation, or build awareness so the prefrontal cortex catches the process earlier. The practical roadmap lives here.
Why you pick even when you want to stop
There's a paradox at the center of all of this. The more you want to stop, the more shame you feel when you don't, and the more shame you feel, the more you pick. This is the part that makes people feel like they're losing their minds.
The shame loop works like this. You pick. You see the damage. You feel guilt, disgust, self-criticism. That emotional state is itself stressful. Stress is one of the most common triggers for picking, alongside boredom and the texture of the skin itself (Grant et al., 2022). So the shame about picking becomes a trigger for more picking. Research on shame in body-focused repetitive behaviors has found it operates as both consequence and driver: people experience shame before episodes (often as a triggering aversive state) and after (which reinforces the cycle and keeps the behavior hidden from anyone who could help) (Houazene et al., 2021; Weingarden & Renshaw, 2015).
This is also why "I should be able to control this" is one of the worst thoughts to keep thinking. It's accurate that you want control. It's not accurate that wanting it harder makes it appear. Each round of self-criticism layers stress on top of an already dysregulated nervous system, and a dysregulated nervous system reaches for its self-soothing tools. Yours happens to be picking.
The shame about picking is part of what keeps you picking. Naming that loop is half the relief.
There's also a deeper layer. For a lot of people, picking isn't "bad behavior with no purpose." It's a self-regulation strategy that works in the short term. It calms a body that runs hot. It focuses a mind that scatters. It gives input to a nervous system that needs input. You're not doing nothing when you pick. You're regulating, just with a tool that costs you a lot. That's worth knowing because it changes the goal. You're not trying to stop "doing a bad thing." You're trying to give your brain a different, less costly way to regulate.
The role of ADHD, anxiety, OCD, and autism
One of the most consistent findings in skin-picking research is high comorbidity with other conditions. Grant and Chamberlain's 2020 U.S. survey of over 10,000 adults found that among those with current skin-picking disorder, 63.4% also met criteria for generalized anxiety disorder, 53.1% for depression, and around a quarter for panic disorder, PTSD, OCD, and ADHD respectively (Grant & Chamberlain, 2020). In-person assessments of smaller clinical samples tend to find more conservative rates, with ADHD around 8% and OCD between 7% and 26% depending on sample (Grant et al., 2022). Autism overlap is less well-studied, but skin picking and other body-focused repetitive behaviors are frequently described in autistic populations as sensory or stimming behaviors.
The pattern across all of these is the same. Picking shows up as a regulation tool for a nervous system that's working overtime in some other way.
In ADHD, the nervous system tends to run under-stimulated when the environment is boring and over-stimulated when it isn't, with poor filtering in between. Picking gives a steady, controllable input that fits both states. It focuses the under-stimulated brain and discharges the over-stimulated one. The full ADHD–picking overlap is mapped here.
In anxiety, picking functions as tension release. The urge often spikes alongside anxious thoughts, and the brief drop in arousal afterward becomes the reinforcement.
In OCD, picking can have a compulsive flavor: an intrusive sense of "wrongness" about a bump or texture, picking to make it right, brief relief, the cycle restarts. This is why excoriation disorder lives in the OCD-related category in the DSM-5, although researchers note it's a distinct condition with its own profile (Grant & Chamberlain, 2020).
In autism, body-focused behaviors often serve sensory and self-regulatory functions, similar to other forms of stimming, with the difference that picking causes tissue damage.
If you suspect one or more of these is part of your picture, you're not pattern-matching for attention. The overlap is real, and treating the underlying condition often reduces picking even when picking wasn't the original target.
What this means for stopping
If picking is a brain mechanism, not a moral failure, then stopping isn't about trying harder. It's about working with the mechanism.
The strongest evidence base is for Habit Reversal Training (HRT), a structured approach that builds awareness of the urge before the action, identifies the triggers and the function the behavior is serving, and substitutes a competing response that delivers similar regulation without the damage. HRT is the first-line behavioral treatment for excoriation disorder (Farhat et al., 2023). Cognitive behavioral therapy, often used alongside HRT, helps with the shame loop and the catastrophic thoughts that follow episodes. Some people also benefit from medication, particularly SSRIs or N-acetylcysteine.
Recovery isn't usually a clean line from picking to not picking. It looks more like episodes becoming shorter, less frequent, and less severe, with longer stretches between them, and a different relationship to the urge when it rises. The goal isn't perfection. It's regulation.
The full how is a separate article: how to stop skin picking, a recovery roadmap. If you want a daily companion that walks you through HRT principles, tracks urges and episodes without judgment, and teaches the science you just read in small daily steps, that's what we built SkinAware for.
Ready to Start Tracking?
SkinAware helps you log episodes, identify patterns, and see real progress over time.
FAQ
Continue Reading
References
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.). American Psychiatric Publishing.
- Farhat, L. C., Reid, M., Bloch, M. H., & Olfson, E. (2023). Prevalence and gender distribution of excoriation (skin-picking) disorder: A systematic review and meta-analysis. Journal of Psychiatric Research, 161, 412–418.
- Grant, J. E., & Chamberlain, S. R. (2020). Prevalence of skin picking (excoriation) disorder. Journal of Psychiatric Research, 130, 57–60.
- Grant, J. E., Dougherty, D. D., & Chamberlain, S. R. (2022). Characteristics of 262 adults with skin picking disorder. Comprehensive Psychiatry, 117, 152338.
- Houazene, S., Leclerc, J. B., O'Connor, K., & Aardema, F. (2021). "Shame on you": The impact of shame in body-focused repetitive behaviors and binge eating. Behaviour Research and Therapy, 138, 103804.
- Weingarden, H., & Renshaw, K. D. (2015). Shame in the obsessive-compulsive related disorders: A conceptual review. Journal of Affective Disorders, 171, 74–84.